|
|
ORTOPEDİA
- Foot
- Foot problems of children
- Orthopedic boot types
writer
Arhitech DİNÇER ÜNAL
İSTANBUL 2004
|
STRUCTURE OF THE FOOT
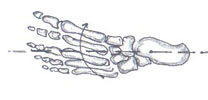
 FOOT SKELETON FOOT SKELETON
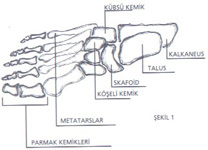
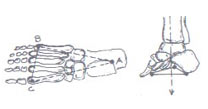
Foot skeleton is composed of 26 bones in three regions, called tarsal, metatarsal and fingers.
Bones in the tarsal region are consisted of seven bones, calcaneus, talus, scaphoideus, cuboideus and, three cornered bone cuneiforme.
Five metatarsal bones are present in metatarsal region.
There are 14 finger bones (phalanx) in the finger region. Among these bones, the ones which link to the comb bones are called linkage bones, the ones in the middle are called mid-bones and the ones in the extremities are called edge bones.
Also, there are two sesamoide bones in first finger and second comb bone joints, formed in declining ages to facilitate the movements
|
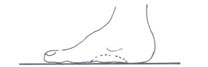
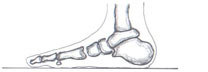
 FOOT ARCS FOOT ARCS
LONGITUDINAL ARC
It is the longitudinal arc present in the medial part of the foot.
The arc length of an adult is 97 mms and the arc height is 17.9 mms.
TRANSVERSAL ARC
It is the arc formed between the first metatars head and fifth metatars head.
The ground contact of a normal foot is shown in figure four.
|
 MOVEMENTS OF THE FOOT MOVEMENTS OF THE FOOT
Movements of the foot:
Are the movements of foot ankle and tarsal and metatarsal joints
Foot ankle movements:
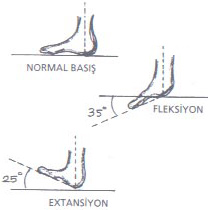
They are mainly consisted of flexion and extension (dorsal flexion).
Flexion angle is 35 degrees, extension angle is 25 degrees. The peaks of these angles are the back part of the foot
|
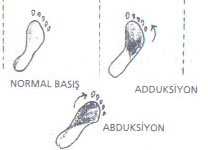 Approach of the metatarsal part to the walk axle is called adduction; secession from the walk axle is called abduction movement. Adduction angle is 30 degrees and abduction angle is 15 degrees.
These angles should be measured in the lateral part of the foot. Approach of the metatarsal part to the walk axle is called adduction; secession from the walk axle is called abduction movement. Adduction angle is 30 degrees and abduction angle is 15 degrees.
These angles should be measured in the lateral part of the foot.
|
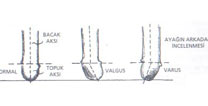
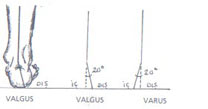 Subtalar joint movements: this is the angle of calcaneus according to the leg axle. The angles of these positions named valgus and varus are about twenty degrees.
Subtalar joint movements: this is the angle of calcaneus according to the leg axle. The angles of these positions named valgus and varus are about twenty degrees.
|
 Shopart joint movements
Shopart joint movements
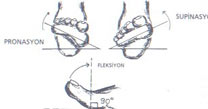
The outer and inner rotation movements of foot basement in the steady state of calcaneus. Outer rotation of the basement is called pronation, the inner rotation is called supination. The angles of these movements are about 20 degrees.
Finger movements: This is especially the flexion movement of the thumb. Flexion angle of the thumb is 90 degrees. The flexion angle reduces towards the fifth finger.
|
 STEP
STEP
Lifting the foot from one point and putting it to a more forward point during the walk is called”step”. The length of a normal step is 65 cms. This length varies according to the leg size of the person and the heel length of the shoe. As the leg length increases, the step length increases, as the heel height increases, the step length decreases.
STEP PHASES (terms)
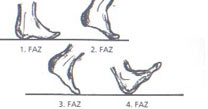
First the heel contacts with the ground, during the walk, the body weight passes from the fifth metatars length to the fifth metatars head and to the first metatars head from here. In this order, one step is completed in four phases.
1. Phase: PRESS this phase is a static phase
2. Phase: LOADING TO THE FRONT PART this phase is a dynamic phase
3. Phase: ATTACK the pushing phase of the body load to the front
4. Phase: BEFORE THE PRESS this phase is the starting phase of the press
|
 THE DISPERSAL OF BODY LOAD:
THE DISPERSAL OF BODY LOAD:
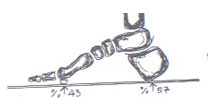
The body weight coming from two legs passes to the ground by the feet. When we put our two feet with ten cms space between them on a cold stone floor, we feel that not every point of our foot contacts the floor with the same load and, some points are in more contact with the floor. These points are the ones which passes the body load to the ground. After this experiment let’s indicate the load dispersal with numbers.
In a naked foot, the load coming from the leg: %57 is in the heel centre, %43 is in the beginning of metatarsus. If the load coming from the leg is P, metatarsus beginning load is M, heel centre load is T, T=0.57P M=0.43 P.
|
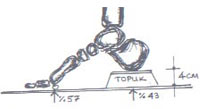 When the shoe is worn, the load dispersal of the body weight changes according to the heel height.
When the shoe is worn, the load dispersal of the body weight changes according to the heel height.
If the heel height is 2 cms, T=0.50P M=0.50P, M=T
If the heel height is 4 cms, T=0.43P, M=0.57P, M>T
If the heel height is 6 cms T=0.25P, M=0.75P,
İf the heel height is more than 6 cms, T=0.10P, M=0.90P
|
 The dispersal of body load in the basement:
The dispersal of body load in the basement:
As mentioned before, the heel load centre is the mid-point of heel diameter. Metatars load is the load condensed in the beginnings of first and fifth metatarsus.
Equivalence triangle:
Triangle formed by the lines uniting the first metatars head, the fifth metatars head and the heel head is called EQUIVALENCE TRIANGLE.
BIOMETRY OF THE FOOT
Biometry of the foot: is the concept and the systems for the analysis of foot sizes.
|
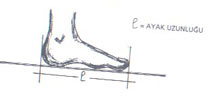 Length of the Foot:
Length of the Foot:
Is the distance between the back heel point and the edge point of the longest finger. Due to the fact that this distance is longer during the loading state, the foot size should be measured while standing up.
|
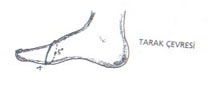 The width of the foot:
The width of the foot:
Foot width called “comb” practically: is around the elips passing from the first metatars head and fifth metatars head.
|
 Generally french pont is used for the size called, number of the foot.
Generally french pont is used for the size called, number of the foot.
French pont is used for the length of the foot, and metric system is used for the width.
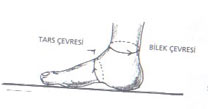
While taking mesurement for the orthopedic shoe, the surrounding of tarsal and ankle part should be measured in addition to the comb size.
|
FOOT PROBLEMS OF CHILDREN
FOOT DISEASES AND DEFORMITIES
In the recent years, sensitivity against the feet and foot diseases have increased. Especially as the parents get more informed on this topic, the foot health controls of children are more intensely performed. Also, as a result of the entry of ladies to the work life, and their wearing high heeled and narrow sized shoes suitable to the fashion, deformations and foot diseases have significantly increased.
In the end of my observations until today, I have observed that especially women wasted time because they tried to cure the pains due to the deformations with analgesics, and they went to an orthopedist in progressive grades. The positive and successful results with consevative therapies are taken in foot diseases if the diagnose is put in time in. In this chapter, I will explain the diagnose methods, foot disease types and conservative therapy methods.
DIAGNOSE METHODS
THE EXAMINE OF WALK:
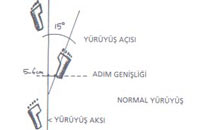
Examination of the walk is a very important factor for the diagnosis of foot deformations. Base deformations affect and form the walk. To examine the walk, it is necessary to know walk axle, foot direction and foot axle concepts.
Walk Axle:
The line uniting the mid-point between the two feet to the point to be reached.
Foot Axle:
The line uniting the heel centre to the second finger axle.
Foot Direction (Step Angle):
The angle formed between the foot axle and walk axle.
After learning the concepts above, let’s observe different walking shapes.
|
 NORMAL WALK:
NORMAL WALK:
During the normal walk, as seen in figure 17, step angle between the foot axle and walk axle is 15 degrees. The distance between heel internal side and walk axle (step width) is 5-6 cm.
|
 THE INTERNAL ROTATED WALK (TOE-IN):
THE INTERNAL ROTATED WALK (TOE-IN):
During toe –in foot axle intersects the walk axle in the front part of the foot and step width increases.
|
 THE OUTER ROTATED WALK (TOE-OUT):
THE OUTER ROTATED WALK (TOE-OUT):
During this walk, step width is variable and the step angle significantly increases.
Toe-in and toe-out walks i mentioned above may be formed due to a deformation in the foot or it may form due to leg-related reasons. Main factors that cause the toe-in walk:
-Pes plana-valgus
-Pes adductus (metatarsus varus )
-tibia curvature
-inversion of femur neck.
During the foot examination, the position of femur and tibia is observed. If the position of these two bones is normal, this means that toe-in has formed due to a foot deformity which is generally pes planum-valgus.
|
 In some pes planum valgus deformities the patient brings his toe to adduction and provides equivalence using its power. Walking does not have the shape of toe-in. The form of foot this way and metatarsus varus are very similar to each other. Therefore, a prescription advised for metatarsus varus(adverse size boot) will certainly do no correction and use.
In some pes planum valgus deformities the patient brings his toe to adduction and provides equivalence using its power. Walking does not have the shape of toe-in. The form of foot this way and metatarsus varus are very similar to each other. Therefore, a prescription advised for metatarsus varus(adverse size boot) will certainly do no correction and use.
|
 In the situation above, if the outer part of the patient’s toe is examined, toughness of the skin can be observed. The reason of this is that the toe inside the shoe is in adduction position all the time and it touches upper side of the shoe.
In the situation above, if the outer part of the patient’s toe is examined, toughness of the skin can be observed. The reason of this is that the toe inside the shoe is in adduction position all the time and it touches upper side of the shoe.
|
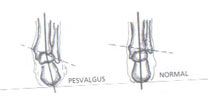
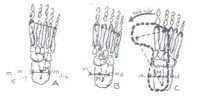 TOE-IN FORMATION DUE TO PES PLANUM-VALGUS:
TOE-IN FORMATION DUE TO PES PLANUM-VALGUS:
In pes planum-valgus heel presses to the interior and the patient brings his foot to toe-in position to provide body-balance. Static meaning of toe-in is shown below figure.
As seen in Figure , in foot “A”; the mid-point of the line uniting the in and out talus bones “M” is present in BALANCE TRIANGLE. This is the press geometry of a healthy foot and the walk of such a foot is normal. In foot “B”, “M” point is out of the balance triangle in medial. In this situation because calcaneus will come to valgus position, pes planum-valgus will be formed in this foot. In foot “C”, to provide balance during the walk, the foot will come to toe-in position.
OBSERVATION OF THE FOOT:
Observation of the foot is done in two ways; with eyes and with hands.
Examination of Foot with Hand:
During the examination by hand, the movements of foot and fingers and, the angles of these movements are evaluated. As a result of this evaluation, pathologic findings are assessed. Examination of foot movements by hand should be performed separately for each foot. The examination of one foot only may be deceiptive for diagnosis. Examination starts with foot ankle movements. The flexion and extension angles of the foot ankle are observed. After this, examination of subtalar joint movements is performed in which the ankle is grabbed with one hand and calcaneus is held with the other hand and calcaneus is brought to varus and valgus. The angle of these heel movements should be 20 degrees according to vertical axle. For the examination of shopart joint movements, heel is held with one hand and metatarsus are held with the other. The foot is brought to pronation and supination respectively. The angles of these movements should be about 20 degrees. Then, the angles of adduction and abduction are examined. The adduction angle must be about 30 degrees; abduction angle must be about 15 degrees. Finally, the finger movements should be examined. In this examination dorsal and plantar flexions of all fingers are examined. In finger examinations, the issue to be most cared is the flexion of the toe which is 90 degrees. If this angle is less than 60 degrees, the situation is pathological.
|
 Examination of the Foot with Eyes:
Examination of the Foot with Eyes:
For the examination of the foot with eyes, two feet with 10 cms space between them and naked up to the knee are pressed on a smooth ground.
-The internal and outer arc are examined. Any disorders in these arcs are noted.
-- The angle between the leg axle and heel axle is examined looking from the behind, varus and valgus position are assessed in the end of this examination.
-By examining the front part of the foot deformations in the metatarsal region and fingers region are assessed.
-Static position of the foot is examined (toe-in, toe-out)
-the appearance of the fingers is examined. With this examination; deformities like hallux-valgus, hallux rigidus, guintus varus, hammer finger can be assessed.
In the end of the examination which are followed the order above, a certain diagnose can be put about foot deformations.
COMPLEMENTARY EXAMINATIONS:
To confirm the previously obtained results and to abolish indecisions, some complementary examinations should be performed.
These analysis are radiography, podography, podoscopy, computerized pressopodoscopy, the analysis of worn shoes, respectively.
|
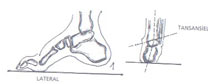
 Radiography:
Radiography:
The condition of the foot is analysed as antero-posterior and lateral. In antero-posterior examination, deformities of fingers and metatarsus are assessed.
In lateral examination, position of the arcs is assessed.
|
 Except the radiographies above, to assess the varus or valgus deformities tangantiel radiography is taken.
Except the radiographies above, to assess the varus or valgus deformities tangantiel radiography is taken.
|
Muhtelif radyografilerin şematik çizimleri :

|
 Podography:
Podography:
Is the image of load dispersal and deformities of the footbase assessed on paper with podograph. The examination with podograph is the most practical and guranteed method of assessing base deformations and the place and rate of body weight that passes to the ground by the base.
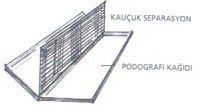
PODOGRAPH: It is a two capped plastic box, in the size enough for a large sized foot base, with a rubber separation in it.
|
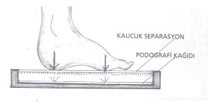 One side of the rubber separation is composed of scanning lines. Fatty Stamp ink is rubbed to this side with the help of a roller. Absorbing podography paper is placed inside the cap on the opposite side of the inky part and separation is closed on this paper. As soon as the foot presses on the separation, a scanning trace is formed on the paper. This trace is the podography of that foot.
One side of the rubber separation is composed of scanning lines. Fatty Stamp ink is rubbed to this side with the help of a roller. Absorbing podography paper is placed inside the cap on the opposite side of the inky part and separation is closed on this paper. As soon as the foot presses on the separation, a scanning trace is formed on the paper. This trace is the podography of that foot.
|
 Although the podograph is a simple device, it gives certain and clear results. In Figure 30 below, normal foot podography is shown. Examples belonging to different foot deformities will be given in the further chapters.
Although the podograph is a simple device, it gives certain and clear results. In Figure 30 below, normal foot podography is shown. Examples belonging to different foot deformities will be given in the further chapters.
|
 Podography paper:
Podography paper:
It must be chosen as especially ink absorbing paper. The sizes should be adjusted in millimetric according to the podograh cover sizes and it should not slide when the foot presses. To be able to state who the podography belongs to, lines must be arranged on the upper part of the paper for necessary information like name, surname, doctor etc.
|
 PODOGRAPHY TYPES BELONGING TO VARIOUS FOOT DEFORMATIONS:
PODOGRAPHY TYPES BELONGING TO VARIOUS FOOT DEFORMATIONS:
In this chapter the characteristics of different podograhies will be examined.
Pes Planus Podography:
In this podography, extension to medial is seen under the longitudinal arc (navicular region).As this extension increases, its grade from base lowness increases.
|
 Pes Planus Valgus Podography:
Pes Planus Valgus Podography:
In this podography; extension is seen in the part under the longitudinal arc but the most significant feature is the convex image in the internal side of the heel and the intensity of the scannings inside the heel.
|
 Pes-Cavus Podography:
Pes-Cavus Podography:
There are no images in the middle part of the foot; the image is present only in the front foot and the heel. Because there is a collapse in the transversal arc in pes cavus, intensity is seen in the scannings of the metatarsal region.
|
 Pes Adductus Podography:
Pes Adductus Podography:
The most significant feature of this podography is the inner rotation of metatarsal region in medial. If there is also valgus deformity, convexity in the heel lateral is found.
|
 Pes-Transversoplanus Podography:
Pes-Transversoplanus Podography:
In this podography, intensity in the scannings of second third and fourth metatars heads is seen.
|
 Hallux-Valgus Podography:
Hallux-Valgus Podography:
In this podography, the edge of toe slides to the lateral, and the head of the first metatars to medial. There is no trace of the second finger or it has a slight trace. Because hallux-valgus generally is formed due to front foot collapse, intensity in metatarsal region scannings is seen.
The information and figures are given belonging to the various diseases mentioned above. Except this, it is necessary to care about two different issues while examinig the podographies.
1-The difference of podography image from normal foot podography
2- Intensity of scannings in pressure points, if this intensity is present in the points normal foot statics require.
A true diagnosis can be put on the foot deformations, after examining these two factors carefully.
It is necessary to performe all the complementary analysis for the diagnosis of foot diseases. If these analyses can not be performed because of some impossibility, at least PODOGRAPHY must certainly be done.
|
 Podoskopi :
Podoskopi :
Podoskopun camına basan ayağın,vitro-pression sonucu,aşırı yükteki noktaların,alt bölümdeki ayna üstüne yansıyan ,sarımsı renkte görüntüsüdür.
|
 Podoscopy:
Podoscopy:
It is the yellowish image of the foot pressing on the glass of podoscope, the overloaded points, reflecting on the mirror in the inferior part as a result of vitro pression.
Podoscope: Podoscope formed from a glass on a curved mirror is developed by Dr. Lelievre and presented in his book named: pathology of the foot. Podoscope is in the height of a normal ladder with a curved situated mirror on the base, and lighting inside, the upper part closed with rough glass in the quality of carrying load.
|
 The results of podoscopy are more optimistic compared to the podography. The results of podoscopy are more optimistic compared to the podography.
For instance
A foot with a podography image of third degree pes planus
gives the image of second degree pes planus in podoscope.
Because podoscopy is formed as a result of the pressure of the foot to the glass, it does not give any certain result in babies and under weighted people. That’s why podoscopy result should be accepted as optimistic and diagnose must be put thinking that the real deformation is a bit more.
Computerized Presso-Podoscopy:
In the recent years, with the progression of technology, there has been changes in podoscope and presso podoscope which shows the foot pressure in more details is produced and presented to medicine use.
The difference of computerized podoscopy from normal podoscopy is the zonal separation of pressure areas by different colours.
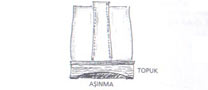
THE EXAMINATION OF WORN SHOES:
When we examine the worn shoes we can have some information about deformations.
Deformities in the foot cause meltings by affecting the heel, base, upper part and the material of the shoe in time.
In the end of the examination by taking care on patient’s duration of using the shoes and the resistance of the materials, the diagnosis of deformations becomes righter.
The affects of deformations on the shoe are given with some examples on the back.
|
 The wearing of the outer milo part on the base stout leather in a sort time indicates that the foot is in over supination.
The wearing of the outer milo part on the base stout leather in a sort time indicates that the foot is in over supination.
|
 Wearing of the heel in the lateral shows that the foot presses on the outer part (varus).
Wearing of the heel in the lateral shows that the foot presses on the outer part (varus).
|
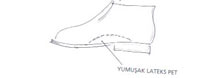
 Convexity of the upper part in medial at first metatarsus head is a sign of hallux-valgus Convexity of the upper part in medial at first metatarsus head is a sign of hallux-valgus
|
FOOT DISEASES AND DEFORMITIES OF CHILDREN
PES PLANUS :
This is a deformity type formed by the collapse of the longitudinal arc of the foot. It may be congenital or it may be caused from the deformations of the foot skeleton (trauma, aseptic necrosis etc), decrease in the load carrying capacity of the foot (muscle weakness, paralysis)
Diagnosis methods:
Examination of the walk: This examination should be done both naked and with shoes on. During the examination, the flexity and softness of the walk, during the steady state it must be controlled if the foot is in adduction. In this deformation, generally the walk is in form of toe in and rarely in toe out image.
|
 Examination of the foot:
Examination of the foot:
-Foot and finger movements are normal during the analysis by hand.
-During the examination done with eyes, when foot shakes, the longitudinal arc is normal but when it presses on the ground arc disappears and the scaphoid protrusion becomes clear.
|
 Radiography
Radiography
It is in the appearance of lateral radiography with a collapsed longitudinal arc and navicular bone close to the ground.
|
 Podography
Podography
The whole trace of the foot base is seen on the podography paper. In third degree pes-planus, the protrusion of scaphoid is significant. The trace of the base gives a concave image in medial.
|
 The examination of the shoes
The examination of the shoes
In the examination of the feet with pes planus; it is seen that the inner side of shoes are melt and the heel is worn out symetrically.
|
 THERAPY
THERAPY
Because pes planus is formed due to various reasons it can be classified like the following;
1-Pysiological base lownnes in babies, this deformity continues until the age of three years
2-As a result of muscle imbalance; base lowness formed due to the collapse of arcs.
3-Congenital plane basement (talus vertical)
4-Pes planum-valgus
5-Base lowness in static valgus position
As a result of the classification above pes planus therapy is divided into two;
1- Conservative treatable base lowness;
2-Operative treatable base lowness
It is unnecessary to treat base lowness of babies until three years old.
Congenital pes planus and static valgus are treated with operation.
Pes planus is treated with conservative method.
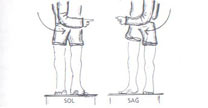
The treatability of base lowness with conservative method can be assessed with the overview on the back page.
The patient stands on podoscop with ten cms space between his feet. The body is turned to right and then to left holding from the waist with the feet steady and hands on both sides. The right longitudinal arc should increase during this. The same movement is repeated by turnig the body to left side. If the longitudinal arcs of both feet respond to this experiment, this patient’s base lowness can be treated with conservative method.
Pes planus treatment of children is done with orthopedic boots.
PES PLANO-VALGUS
When the foot is loaded talus moves to medial and plantar, makes a valgus deformity by pushing the calcaneus to outer side. As a result of this the longitudinal arc in medial becomes straight. The deformation formed like this is called pes plano-valgus.
|
 Diagnose methods:
Diagnose methods:
Examination of the walk
As a result of the sliding of leg weight point to medial, the leg turns to inner side to provide the balance and toe-in walk is formed this way.
|
 Examination of the foot
Examination of the foot
-During the examination with hand, the foot and finger movements are normal.
-During the examination with eyes, longitudinal arc is collapsed. During standing, toe is in adduction, slide in leg axle is seen, when looked from behind (valgus).
|
 Radiography
Radiography
The situation of scaphoid is like in pes planus. Talus is in crop position and calcaneus is in valgus position.
|
 Podography
Podography
The whole trace of the base is out. The traces in heel medial and the head of first metatars are more significant.
|
 The examination of shoes
The examination of shoes
The internal head and heel medial have melted. As a result of the collapse of fort,the upper part has lied towards medial.
Treatment
Heel internal daggered and scaphoid peded boots are recommended. If the walk is toe-in,then pronator dagger is added to these orthesis.
CONGENITAL PES PLANUS (talus vertical):
It is a congenital foot deformity.
Diagnose methods:
Examination of the walk: The walk is generally normal but rarely is toe-out.
Examination of the foot:
The foot movements are limited. Base is in a convex appearance and the foot is in dorsal flexion (in neonatal babies). Front foot is in pronation, back foot is in valgus position.
|
 Radiography Radiography
Talus is in vertical position in lateral graphy. Calcaneus is in supination position. Talus neck has slided under the navicular bone.
|
 Podography
Podography
The whole trace of the base is out. Traces in Kamara are more intense.
Treatment:
Early treatment is necessary. Pronation and dorsal flexion of the foot, adduction of the front foot, and plantar flexion of calcaneus are corrected with hand and gets bandaged. If the necessary correction can not be provided with this method, operative method should be applied as soon as possible.
PES CAVUS (HOLE BASE):
This is a deformity in which longitudinal arc of the foot increases. Generally it is caused by congenital reasons, in some cases it is formed as a result of muscle imbalance caused by neurological disorders.
Diagnose methods:
Examination of the walk:
Walking is generally normal.
|
 Examination of the foot:
Examination of the foot:
The longitudinal arc of the foot is generally increased and the length is decreased. There is pow situation in the fingers and the foot back is bumped. Callus formation and toughness are seen in metatars heads. There is callus formation in interphalangeal joint. The front part of the foot is in pronation and plantar flexion, mid-part is in supination and dorsal flexion.
|
 Radiography: In lateral radiography metatars heads are collapsed and calcaneus is too vertical. Hyperextension in metatarso-phalangeal joint and flexion in distal-inter-phalangeal joint.
Radiography: In lateral radiography metatars heads are collapsed and calcaneus is too vertical. Hyperextension in metatarso-phalangeal joint and flexion in distal-inter-phalangeal joint.
|
 Podography:
Podography:
Kamara part between the front foot and heel has disappeared. Scannings in metatars heads are significant, scannings in finger pressure points are insignificant.
|
 Examination of the shoes
Examination of the shoes
The points under metatars heads in the base are more worn out compared to the other parts, in some events stout rubber is pierced.
Treatment:
Conservative therapy with special orthopedic boot is done (boot for pes cavus).
PES ADDUCTUS (SICKLE FOOT-METATARSUS VARUS):
It is a foot deformity which is generally seen in both parts. It is hereditary or may be formed after pes planus equinovarus deformity. In this disease the front part of the foot is in adduction. The longitudinal arc of the foot is collapsed and cuboid part has become significant.
Diagnose Methods:
Examination of the walk:
Walk is in TOE-IN position
Examination of the foot:
Front foot is in adduction, back foot is in valgus and the longitudinal arc is collapsed.
|
 Radiography:
Radiography:
In A-P graphy, the rotation of metatars to medial is significant.
|
 Podography:
Podography:
It looks like pes planus podography. The trace of the first metatars head is separated from the other metatars heads, and is out of the normal foot contour. The first finger trace is separated from other finger traces. Concave image is present in heel lateral.
|
 Examination of the shoes:
Examination of the shoes:
Upper parts of the shoea are worn out in internal part towads medial. The under part of the toe and medial part base have melted.
Treatment:
Correction with the help oh hand and bandage is done on babies and little children. In further ages night atel and adverse size boots are necessary. (look; adverse boot for metatars varus, ort.boot)
PES EQUINO-VARUS (CONGENITAL BENT FOOT):
The foot deformity which may be congenital or acquired. The foot can not be brought to passive or active dorsal flexion.
Diagnose Methods:
Examination of the walk:
The heels do not touch the ground while walking.
Examination of the foot:
The foot can not be brought to dorsal flexion and pronation during the examination with hands. During the examination done with eyes, foot is in plantar flexion and supination, shopart joint is in adduction (metatarsus varus). Longitudinal arc is increased and calcaneus is in varus position.
|
 Radiography:
Radiography:
In lateral radiography angle between talus and calcaneus axles is decreased. In tangantiel graphy varus is assessed.
|
 Podography:
Podography:
The trace of the front part and lateral of the foot is significant, the heel trace is either little or does not exist. The outer part of the foot (lateral) makes a convex trace.
Examination of the shoes:
In advanced cases the shoes of walking children are deformed. The front part turns inside and outer parts of nose melts. Base or upper part is pierced, and the heel is not worn out.
Treatment:
Correction with hand is done and fixation with bandage is done. After a complete correction, the foot is fixed with a saint germaine atel. After the patient starts walking, treatment is continued with outer longitudinal daggered, low adverse thomas heeled, adverse size boots. In such orthopedic boots scaphoid ped is not placed and the inside of the base is left empty. (look:equino-varus ort.boot)
PES CALCANEO-VALGUS (CONGENITAL HEEL FOOT):
This is a congenital deformity in one or two feet. This disease which is formed as a result of gene failure is formed as a result of the dominance of dorsal extensor muscles to plantar flexor muscles.
Diagnose methods:
Examination of the walk:
Because deformity is congenital examination of the walk is impossible in babies.
|
 Examination of the foot
Examination of the foot
In the examination with hand: The foot resists while being brought to supination or dorsal flexion.
In the examination with eyes: The foot is in slight pronation and too much dorsal flexion and its back is close to tibia, the longitudinal arc has disappeared.
Radiography:
In lateral radiography the bones are in normal shape. Calcaneus has become vertical.
Podography:
In advanced case the trace of vertical foot does not appear in podography
Treatment:
In early cases correction is done with hand, in one or two month old cases, the foot is bandaged after the correction with hand. The treatment is operative between 1-12 ages. To assist the treatments, high thomas heeled high scaphoid pedded, longitudinal internal daggered, normal size orthopedic boots are recommended.
|
|
ORTHOPEDIC BOOT TYPES
|
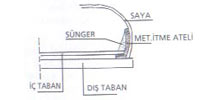
 FIRST STEP BOOT: In babies, the kind of boot which is suitable after the “ranking” starts. In this type, soft leather, and thin base insert should be used for the foot movements to be comfortable. To enable the flexion and extension of the fingers, the nose part of the size should be high. Especially, between 17-19th numbers flexible upper parts should be used. The most suitable material for this is 33 mm sponge rubber or french cattle leather.
FIRST STEP BOOT: In babies, the kind of boot which is suitable after the “ranking” starts. In this type, soft leather, and thin base insert should be used for the foot movements to be comfortable. To enable the flexion and extension of the fingers, the nose part of the size should be high. Especially, between 17-19th numbers flexible upper parts should be used. The most suitable material for this is 33 mm sponge rubber or french cattle leather.
Babies’feet are generally fat. Also they can not help while wearing their boots, by giving shape to their feet. On the contrary, they sometimes bring their feet to plantar flexion as a reflex and harden wearing to facilitate wearing: the models with porteriz in the front should be stilized.
|
 After the babies start walking they have plane base for an average time of two years. The first step boots to be used in this period should certainly not be inserted tough internal support (scaphoid pad), on the contrary latex pad which can apply massage to base muscles should be preferred. If the tough pad is used, medial muscles are becoming lazy and they cause pathological plane base in the future. There is no drawback in not using arc support in first step boot. After the babies start walking they have plane base for an average time of two years. The first step boots to be used in this period should certainly not be inserted tough internal support (scaphoid pad), on the contrary latex pad which can apply massage to base muscles should be preferred. If the tough pad is used, medial muscles are becoming lazy and they cause pathological plane base in the future. There is no drawback in not using arc support in first step boot.
|
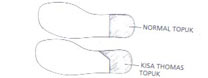 Soft material should be used in first step boot heels, normal heel or short contact heel should be used as type.
Soft material should be used in first step boot heels, normal heel or short contact heel should be used as type.
|
 One of the important units of first step boots is the shoelaces. Babies generally solve the shoelaces while playing with them and they may fall down by pressing on them. To avoid this shoelace height should be very well adjusted. Before linking the shoelaces, the internal and outer height of them in loose position must be less than gamba position. One of the important units of first step boots is the shoelaces. Babies generally solve the shoelaces while playing with them and they may fall down by pressing on them. To avoid this shoelace height should be very well adjusted. Before linking the shoelaces, the internal and outer height of them in loose position must be less than gamba position.
|
 NORMAL ORTHOPEDIC BOOT: NORMAL ORTHOPEDIC BOOT:
It may be used as protective orthopedic boot as well as it is advised for pes planus. Generally in normal orthopedic boot produced between 21-30, tough fort is used in middle tough convex and flexiple upper part. To help the flexibility of the upper part, vardola must be turned from the 25 number. The highest point of the fort should be left under the hanged points. In this kind of orthopedic boots, arc support should be used as 4-5 mm till number 25;6-8 mm till number 30. Ideal material for arc support (foam rubber) is foam rubber or mushroom. As size the size with high nose and large comb should be preferred. As heel, short type thomas heel is the most convenient form. Ideal materials are; videla leather in the upper part, flexible thermorubber or leather.
|
 DAGGERED (FINTA) ORTHOPEDIC BOOT
As we have seen in the previous orthopedic boot units, dagger is the part between the leather and uste for the treatment of foot diseases and to create different heights in some parts of the shoe base. Daggers are divided into two parts according to direction as INTERNAL DAGGER (medial), OUTER DAGGER (lateral) and according to their usage as heel dagger, longitudinal dagger and pronation dagger. Heel daggered boot: It is the orthopedic boot inserted in the internal part of the boot heel, regulated with dagger. As advised for pes planus valgus, it can also be used for aseptic treatment in navicular bone. The heel internal dagger is also called as varus dagger because it corrects valgus deformity. Heel internal dagger may be used directly in to the boot as well as between the heel and uste. DAGGERED (FINTA) ORTHOPEDIC BOOT
As we have seen in the previous orthopedic boot units, dagger is the part between the leather and uste for the treatment of foot diseases and to create different heights in some parts of the shoe base. Daggers are divided into two parts according to direction as INTERNAL DAGGER (medial), OUTER DAGGER (lateral) and according to their usage as heel dagger, longitudinal dagger and pronation dagger. Heel daggered boot: It is the orthopedic boot inserted in the internal part of the boot heel, regulated with dagger. As advised for pes planus valgus, it can also be used for aseptic treatment in navicular bone. The heel internal dagger is also called as varus dagger because it corrects valgus deformity. Heel internal dagger may be used directly in to the boot as well as between the heel and uste.
|
 The dagger height must be very carefully adjusted. Dagger higher than necessary may cause a huge varus deformity in spite of the desired treatment.
The dagger height must be very carefully adjusted. Dagger higher than necessary may cause a huge varus deformity in spite of the desired treatment.
|
 If the heel internal dagger height is more than some height for some reason and if the heel part is moving inside the boot, a rubber spur should be inserted inside the boot, in heel lateral touching the fort,to avoid valgus deformity increase.
If the heel internal dagger height is more than some height for some reason and if the heel part is moving inside the boot, a rubber spur should be inserted inside the boot, in heel lateral touching the fort,to avoid valgus deformity increase.
|
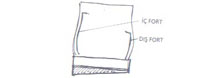 The shape and height of the boot are very important factors each, in internal heel daggered boot.asymetric fort or t-fort is used as shape.fort height should certainly not be on the talo-calcaneal joint line. Especially if the fort height on the medial has passed the knuckle bone point and reached the tibia, melting will occur in tibia because of the pressure on this last point.
The shape and height of the boot are very important factors each, in internal heel daggered boot.asymetric fort or t-fort is used as shape.fort height should certainly not be on the talo-calcaneal joint line. Especially if the fort height on the medial has passed the knuckle bone point and reached the tibia, melting will occur in tibia because of the pressure on this last point.
The boot manufactured by inserting the dagger to the outer part of the heel is called heel outer daggered boot. This type is generally recommended for the treatment of varus deformity.
Longitudinal daggered boot:
The boot formed by dagger inserted from the heel to the nose of the shoe and the boot. It can be separated into two according to its position as internal and outer.
Longitudinal internal daggered boot: although it is generally advised in pes planus valgus disease,when the valgus deformation is much and toe in has increased, recent researches have found out that this treatment is certainly wrong. Let’s try to explain the negative effects of longitudinal internal dagger in treatment.
-The internal dagger inserted longitudinally causes extra supination.
-Reduces the flexion by toughening the base of the foot because it covers the base longitudinally and limits the flexion this way.
-Causes toe-in to increase by raising the internal part of the heel supported by hard fort with dagger.
-May cause the tibia bones of little patients using this kind of shoe or boot to bend.
Because of the reasons we tried to tell above, heel internal daggered and pronation daggered boot should be recommended instead of longitudinal dagger in pes planus valgus. Longitudinal internal dagger must especially be used in toe-out situation.
|
 Longitudinal outer daggered boot: it is the boot formed by inserting on the outer part (lateral) of the shoe with finta to correct pes planus equino varus and the curveness of tibia formed in babies because of rachitism or other reasons. Longitudinal outer daggered boot: it is the boot formed by inserting on the outer part (lateral) of the shoe with finta to correct pes planus equino varus and the curveness of tibia formed in babies because of rachitism or other reasons.
|
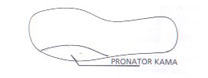 Pronator daggered boot:
Pronator daggered boot:
: the dagger inserted on the base lateral,in the mid-point of outer mylo point in the form of ½ elips to correct the supination in front of the foot. Ideal and functional pronation dagger is showed in figure
|
 The ideal boot type for toe in correction is the pronation daggered boot. The boot produced by using pronation dagger and heel internal dagger is the most positive boot type for pes planus valgus treatment.
The ideal boot type for toe in correction is the pronation daggered boot. The boot produced by using pronation dagger and heel internal dagger is the most positive boot type for pes planus valgus treatment.
|
 General Information about Daggered Boots:
General Information about Daggered Boots:
Daggers should be made of tough and flexible material. The most suitable material for this is real stout leather, also thermorubber or neolit can be used. During the production the sizes assessed by the doctor must be used and calipers should be used to provide sensitivity. Longitudinal daggers should not cover the whole base and must become zero in the base axle.
|
 Heel internal and outer dagger can become zero in medial or lateral by covering the whole base.
Heel internal and outer dagger can become zero in medial or lateral by covering the whole base.
|
 Pronation dagger should not be more than the base axle not to block the flexibility of the base.
Pronation dagger should not be more than the base axle not to block the flexibility of the base.
|
 Camber in daggered boots: It is same as the other orthopedic boots but fort has different features. The purpose in these boots is to make the internal or outer pressing foot press vertically. While doing this with the help of dagger, body load makes more pressure on the forts than normal. So,the fort should be hard and resistable. Asymetric or t-fort should be preffered in forts as shape. ın finta boots,size is very important. While preparing the size, the part behind the cadian should be pulled 1/2 number small to avoid calcaneus move in the boot.
Camber in daggered boots: It is same as the other orthopedic boots but fort has different features. The purpose in these boots is to make the internal or outer pressing foot press vertically. While doing this with the help of dagger, body load makes more pressure on the forts than normal. So,the fort should be hard and resistable. Asymetric or t-fort should be preffered in forts as shape. ın finta boots,size is very important. While preparing the size, the part behind the cadian should be pulled 1/2 number small to avoid calcaneus move in the boot.
In longitudinal and pronation daggered boots, vardola should not be used for the flexibility of the base.
|
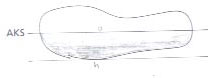
 ORTHOPEDIC BOOT FOR PES CAVUS
ORTHOPEDIC BOOT FOR PES CAVUS
The shoe recommended for pes cavus in the children must be boot. In this type of boot, the insertion and the shape of the pads to be applied on the base is just the same as pes cavus base. Fort and camber is like in the normal orthopedic boot. Normal form in heel should be preferred. If there is lying in calcaneus axle; (valgus-varus), internal or outer dagger can be inserted to the heel part of the boot.
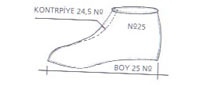
The tarsal part of the foot has made camber in pes cavus. To press this camber, the contrpie part of the boot must be done more narrow compared to the normal boot. So, while preparing boot size for pes cavus, contrpie part shoul be pulled 1/2 number smaller.
|
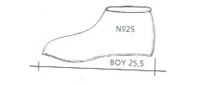 As a result of the pressure on tars region, the length of the foot will increase a bit. Because of this, the size length must be pulled 1/2 number larger in the front part.
As a result of the pressure on tars region, the length of the foot will increase a bit. Because of this, the size length must be pulled 1/2 number larger in the front part.
|
 In pes cavus boot, the front parts of gambas (upper contrpie) should be more open than normal, so, pressure can be applied on the tars bones by more tense links. (Figure 20) As shoelace, thick mercerised shoelaces should be preferred.
In pes cavus boot, the front parts of gambas (upper contrpie) should be more open than normal, so, pressure can be applied on the tars bones by more tense links. (Figure 20) As shoelace, thick mercerised shoelaces should be preferred.
|
 Because of the reason we explained above gambas should be extended to the mylo point to link the boot better. Because of the reason we explained above gambas should be extended to the mylo point to link the boot better.
For the treatment of pes cavus in ladies low and large shoes should be made and pes cavus base should be inserted.
|
 ADVERSE SIZE BOOT
ADVERSE SIZE BOOT
It is the boot type recommended for pes adductus and pes planus equinovarus congenitus. Before giving the necessary information about adverse size boot, let’s explain the difference between metatarsus varus and toe in (internal rotated press). Metatarsus varus and toe in give similar images during the walk. The difference between them is that metatarsus varus is internally rotated in the metatarses and in toe in foot is internally rotated from the ankle.
These two deformations should not be confused with eachother and the foot must be very carefully examined. While writing the boot prescription, adverse size should certainly not be recommended for toe in. Metatars of the foot in toe in position is generally in its axle. Adverse size causes other deformations by forcing metatarses in normal position to abduction. The most positive method To avoid the confusion above is A-P foot radiography. So, metatarsus varus can certainly be assessed.
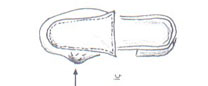
Adverse size boot for metatarsus varus:
The most important units to be attended in adverse size boot production are size, fort, camber and heel.
The most important therapeutic factor of the adverse size boot is the outer rotated shape of the size in metatarses. The rotation angle of the form which should push the metatarses outwards is assessed according to the situation of the disease.
Half adverse size is used when the metatarsus varus is low and complete adverse size is used in advanced situations.
|
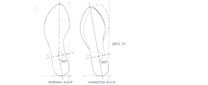 HALF ADVERSE SIZE
HALF ADVERSE SIZE
It is the symetric size shape.
|
 COMPLETE ADVERSE SIZE:
COMPLETE ADVERSE SIZE:
The size type recommended when the varus in metatarses is prominent.
|
 Fort-camber:
Fort-camber:
The fort shape in adverse size boot is asymetric fort as we saw in normal size boot before. But fort is extended up to first metatars in medial.
Camber has a different form. While the fort extended to the first metatars pushes metatarses outwards, it produces valgus position in the toe.
To reduce this, cambers should be made of soft material and next to the toe should be left empty in medial.
Heel:
Normal heel or short type heel should be used not to increase adduction.
|
 Ortez
Ortez
The shape and position of the ortez is adjusted according to the foot shape and deformation in the adverse size boot produced for pes adductus.
During supination, 4-6 mm high pronation dagger is inserted to the outer part of the front base.
|
 -during pronation no ortez is necessary. If there is valgus in the heel (very often), 4-6 mms high heel internal dagger is inserted. This dagger also reduces the pronation in the front foot.
-during pronation no ortez is necessary. If there is valgus in the heel (very often), 4-6 mms high heel internal dagger is inserted. This dagger also reduces the pronation in the front foot.
-to push the metatarses, in medial of metatarses, metatarsal pushing atel is placed.
. The part of this atel made of hard stout leather touching the foot is covered with soft rubber or sponger to avoid injury in the skin.
|
 In the metatarsal pushing atel replaced boot, to keep the balance of the back foot (posterior), “tarsal back pushing”device should be placed to the front part of cuboid and calcaneus In the metatarsal pushing atel replaced boot, to keep the balance of the back foot (posterior), “tarsal back pushing”device should be placed to the front part of cuboid and calcaneus
|
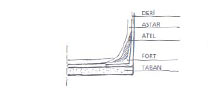 French cattle stout leather should be used in the production of atels above. To make atel work well, it must be sized entering between the upper part of leather and base lining. (Figure 29) Also by shaving the upper parts of the atel, the skin injury is avoided. French cattle stout leather should be used in the production of atels above. To make atel work well, it must be sized entering between the upper part of leather and base lining. (Figure 29) Also by shaving the upper parts of the atel, the skin injury is avoided.
Adverse size boot does not look nice. To make this boot like the children would be reluctant to wear, more sympathetic, it is necessary to be very careful while choosing the model.
|
 ADVERSE SIZE BOOT FOR PES EQUINO VARUS
ADVERSE SIZE BOOT FOR PES EQUINO VARUS
While producing adverse size boot for this disease, longitudinal outer dagger is added different from the previous ones. While correcting the varus in heel with longitudinal dagger, toe in correction is assisted. Long thomas heeling piece is placed adverse to the heel part. The heel length is the half of normal orthopedic boot heel length. (Figure 30) Scaphoid pad is certainly not placed.
|
|
|
|




